
To date, almost everything I know about sitting disabilities has been anecdotal. And while the anecdotes I’ve heard online or in direct communication have been wonderfully enlightening, I was never sure which experiences were representative, and which were singularities.
In order to get a more accurate view, I created a general survey on sitting disabilities, which I unleashed on the Sitting Disabilities Facebook group on July 13th, 2020. After a week, I closed the survey and collected the results, which I summarize here.
Fourteen individuals responded. While that’s not a huge number, it was enough to discover some commonalities and unearth some general trends.
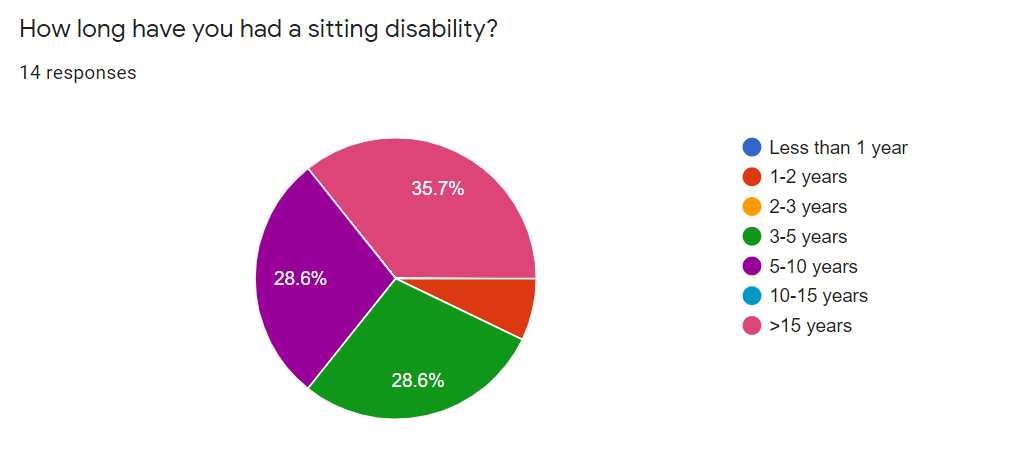
Length of Sitting Disability
I wasn’t surprised to see that only one responded reported having a sitting disability for less than three years. My suspicion (which I have no data to support) is that someone with a recently manifested sitting disability would not be keen to use the phrase “sitting disability,” nor to join an online support group, or take a survey.
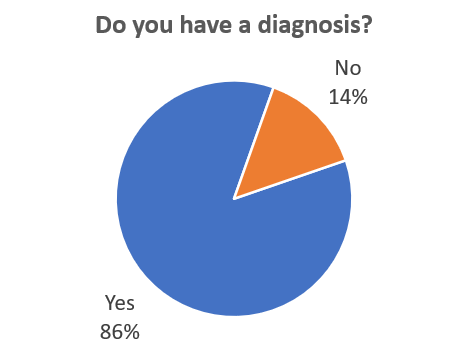
Diagnosis
I was surprised – and heartened – by the number of respondents who had a diagnosis. While there’s no such thing as a good sitting disability, there’s a certain comfort in being able to apply a label to your condition. At the very least, it makes it easier to explain your condition to other people.
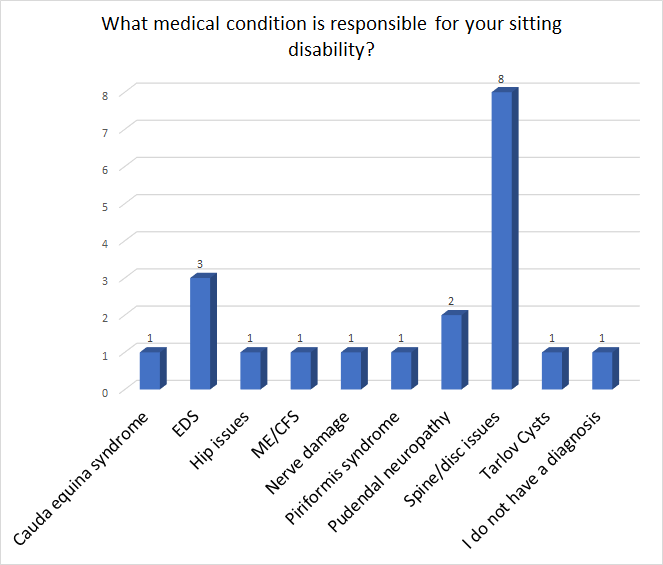
Spine and disk issues were by far the most common diagnosis. The second-most-common diagnosis was a write-in: Ehlers-Danlos syndrome (EDS). EDS is actually not a single disease, but a cluster of genetic conditions that affects connective tissues, and often leads to hypermobile joints and stretchy skin. People with EDS are predisposed to develop additional health problems. Interestingly, each survey respondent who selected EDS also had some kind of back condition.
The third most common condition was pudendal neuropathy, which is a catch-all term for a number of conditions that cause pain in the pudendal nerve (which runs between the anus and the genitals).
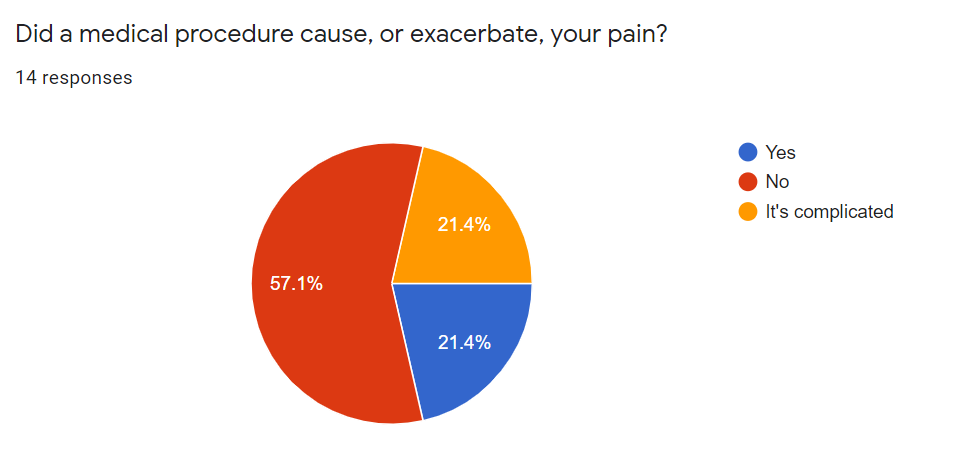
Medical Procedures & Sitting Pain
I have long suspected that most of the treatments I endured for back pain didn’t help, and possibly made things worse. I have also heard whispered anecdotes of botched procedures that left patients in more pain than they started with, but I had no idea whether that was a common occurrence or a rarity. I included a question on the survey to find out.
Fortunately, the majority of respondents did not suffer as a result of medical procedures. But a sizeable minority (six out of fourteen respondents) answered either “Yes” or “It’s complicated.” The results didn’t help much to set my mind at ease.
Those who answered “Yes,” or “It’s complicated” were asked for details. I had planned to summarize the answers, but I didn’t trust myself to properly represent their experiences. So instead, I’m reproducing the (anonymous) answers in their entirety.
Medical Procedures and Sitting Pain
Please list any relevant details about the medical procedure you underwent, and how that affected your sitting pain.
4 responses
- Went to a chiropractor who didn’t run any scans before doing manual adjustments. He made it way worse.
- I’ve had an herniated disc L5S1, after a year went to two operations. First one did nothing, second time I woke up in hell. After years I found out I probably had an haemorrhage with the second surgery which caused Cauda Equina Syndrome. I was 30 years old and was told I was too young to have these back issues. Last year I’ve learned I’ve got EDS which probably caused my back issues
- Hysterectomy due to misdiagnosis delayed proper treatment. Resulted in permanent pelvic muscle dysfunction
- Unguided Lumbar Puncture in Severe Congenital Stenosis case leading to intrathecal blood pool and adhesive arachnoiditis
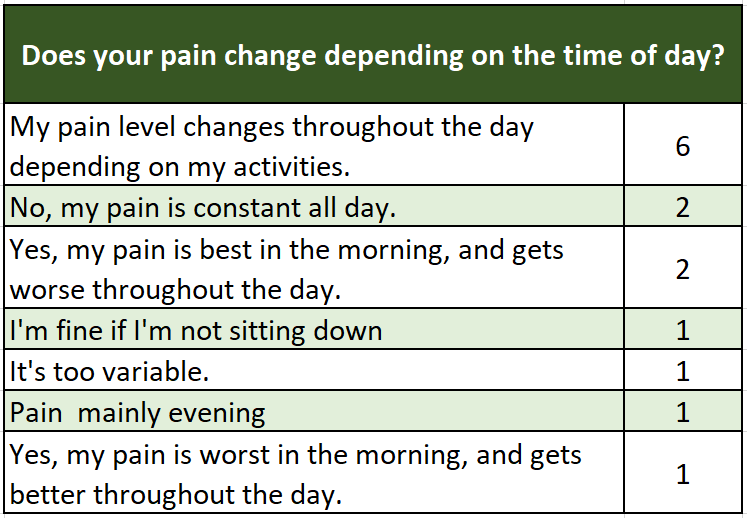
Pain Patterns
I was curious to see if sitting pain fell into any discernable patterns beyond, y’know, existing when a person sits down. So I asked about daily pain patterns.
I expected pain patterns to track with specific diagnoses, but this wasn’t the case at all. Pain patterns seemed completely independent of the underlying cause. The most common answer was, “My pain level changes throughout the day depending on my activities.”
Pain Triggers
Next, the survey asked, “Do you have any pain triggers, besides sitting?” Here, I did see a weak correlation between diagnosis and pain triggers, although there weren’t enough respondents to draw conclusions for any condition except spine/disc issues.
Four respondents with spine/disk issues reported pain when they engaged in activities that compressed the spine (such as jumping, running, or carrying heavy things), while three respondents reported problems with bending or stooping.
There were no discernable patterns for those with EDS or pudendal neuropathy.
Other reported pain triggers include:
- Standing too long
- Walking uphill
- Bowel movements
- Weather (especially cold weather)
- Lying in bed (particularly if pain is on one side)
- Twisting
- Fatigue
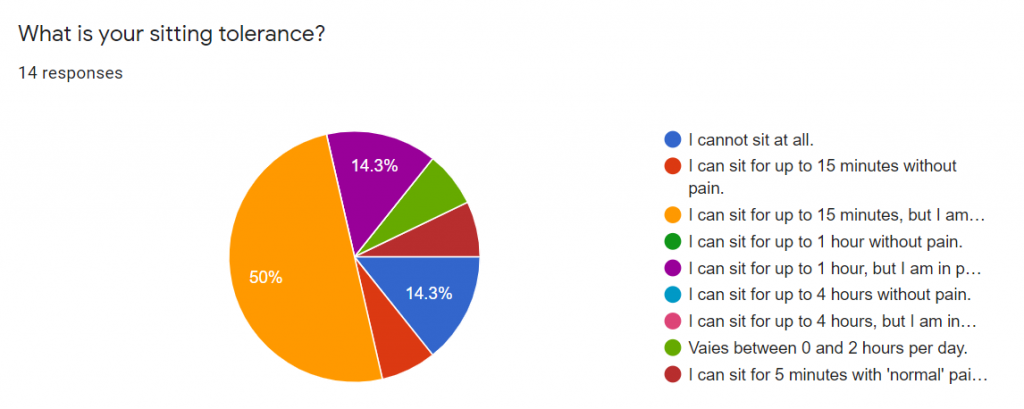
Sitting Tolerance
I included a question about sitting tolerance, where I rather optimistically listed time periods of up to four hours.
It turns out that the maximum reported tolerance of any respondent was two hours – and only on a good day. Eleven respondents reported a tolerance of fifteen minutes or less.
Capabilities
I personally spend a lot of time whining about all the things I can’t or won’t do anymore, and I was curious to see whether any other sitting-disabled folks had miraculously found a way to carry on. In general, the answer is no.
The most difficult activities were traveling by airplane, and going to movies/concerts/plays. Going to restaurants and visiting friends were both more manageable prospects, although apparently neither one could be done on a lark.
I was surprised to see that traveling by car was ranked as one of the more manageable activities. Opinions on public transit were more scattered.
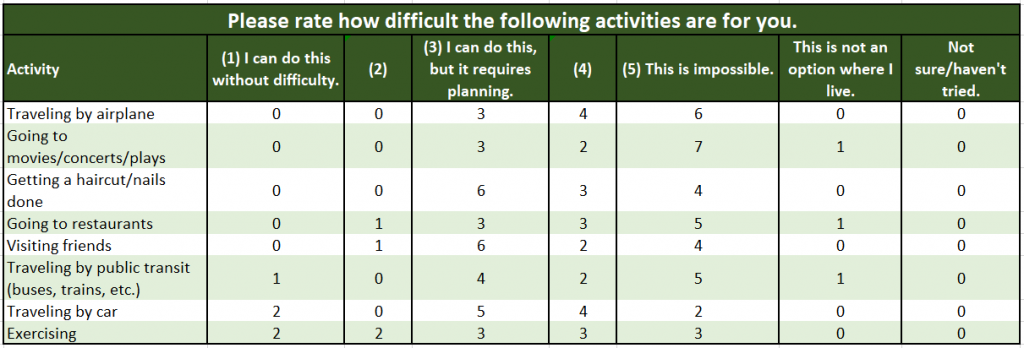
“Exercising” was the activity that showed the greatest spread in difficulty rankings. Four respondents found it relatively easy to manage, which means that exercising was, on average, the easiest activity on the list for people to engage in.
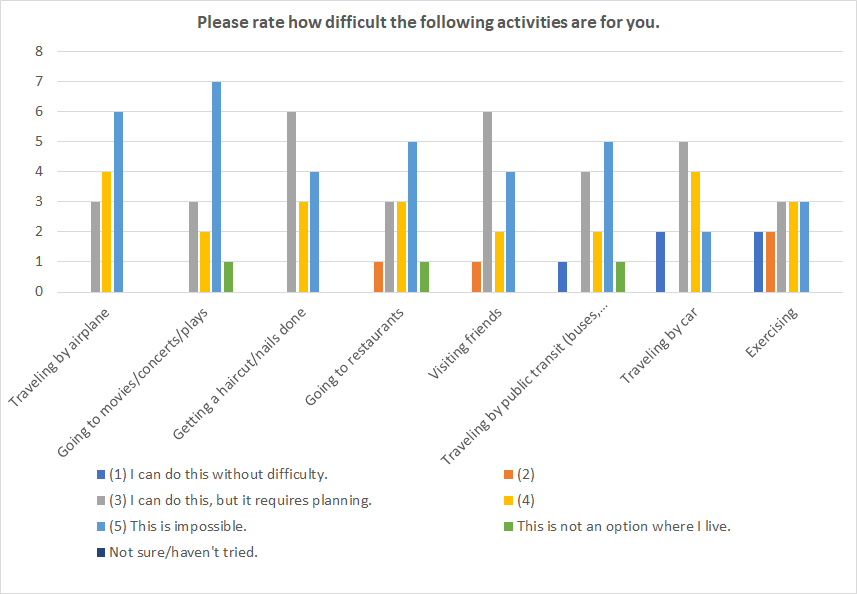
Since that graph is tough to read, I’m including a table as well.
Long Form Questions
Building this survey was a stab in the dark, as I had to guess which questions would solicit meaningful responses, and anticipate which answers participants might choose. But I left some questions open-ended, an acknowledgement that I do not know what I do not know.
What do you miss most about your pre-sitting disability life?
One respondent summed the matter up succinctly – “Everything”. The major recurring theme among the answers was how much participants missed normal life.
Five respondents listed travel, whether it be road trips, or a quick run to the grocery store. Four missed being able to socialize with others. Concerts, festivals, movies, and even card games at the dining room table were now off-limits.
Three respondents missed being able to participate in athletic activities, while another three missed sitting itself. It turns out there isn’t a sitting-disability-friendly alternative to lounging on the couch.
Perhaps my favorite answer was the pointedly specific, “Not being harassed on transit by elderly people who don’t believe I have a disability.” I don’t know why the elderly in this respondent’s orbit are so curmudgeonly, but I certainly understand the difficulty of proving a disability to strangers when you’re young and healthy-looking.
EDIT: The writer of this comment explained that she often needs to ride in the section of the subway reserved for elderly or disabled individuals. In order to ride comfortably, she arranges her things across two seats. Although she carries a button that reads, “My Disability Is Invisible,” a handful of elderly riders have taken it upon themselves to vigorously defended an empty seat from her encroachment.
If you could solve any single problem related to your sitting disability, what would it be?
One general category clearly stood out – Travel. Five respondents missed driving, two missed being able to fly comfortably in coach, and two missed travel in general.
One participant missed work (and the financial security that comes with it), while another had solved the puzzle by insisting their workplace provide them with a reclining chair.
Some of the responses were even more modest. “Anything would be a massive bonus,” wrote one participant, while another only asked to, “Be free of pain.”
Solutions
I often get annoyed when well-meaning bystanders try to offer up a solution to my back problems, without really understanding my problem in the first place. But I still want solutions, and figured maybe my fellow sufferers had stumbled upon coping mechanisms that hadn’t occurred to me.
Which treatments or therapies help you manage your pain?
This was another question where I expected the answers to correlate to the underlying condition, but again I was wrong.
It turns out exercise was the most common therapy used. Four respondents went to physical therapy (or physiotherapy, depending on the country). Others walked, swam, or just kept moving. One reported that bracing helps. (Although a definition was not provided, I assume “bracing” refers to the strategy of stiffening the torso muscles during certain movements to protect the spine.)
Five respondents reported that medications were part of their treatment toolkit. The meds used included NSAIDs, opioids, Lyrica, baclofen, and GABA. One resourceful individual used, “Every pain med known to medical science.” Two respondents relied on medical devices – one on a spinal cord stimulator, the other one on a dorsal root ganglion spinal stimulator.
Three respondents reported using heat and ice. Others used alternative treatments, like chiropractic sessions, meditation, and massage. One used an acupressure mat, which I only just learned was a thing.
Several respondents emphatically noted that not sitting down was key to managing their pain, an observation which should surprise no one.
Are there any sitting-pain-related products that you find indispensable?
It’s nice when you can throw money at a problem and make it go away. The products that sitting-disabled respondents reported using ranged from the high-end (such as this super-cool looking Varier Move chair, a custom-made flat wheelchair, and an electric standing scooter), to the everyday (such as heat and ice packs, and a laptop lap tray from IKEA).
Three respondents reported using zero-gravity chairs, while two others used reclining chairs. Two respondents Cushioned Their Assets.
Four participants used standing desks, although in one case, “standing desk” equaled “high counter.” One individual reported rigging up their own standing desk. Details were not given, but I’ve personally rigged up standing desks using ironing boards, stacked suitcases, window ledges, and a coffee table with sawed-off legs set on top of a regular desk.
Other products included:
- A shower bed
- TENS machine
- Back brace
- Adjustable bed frame with zero-gravity setting
- Grocery cart
Demographics
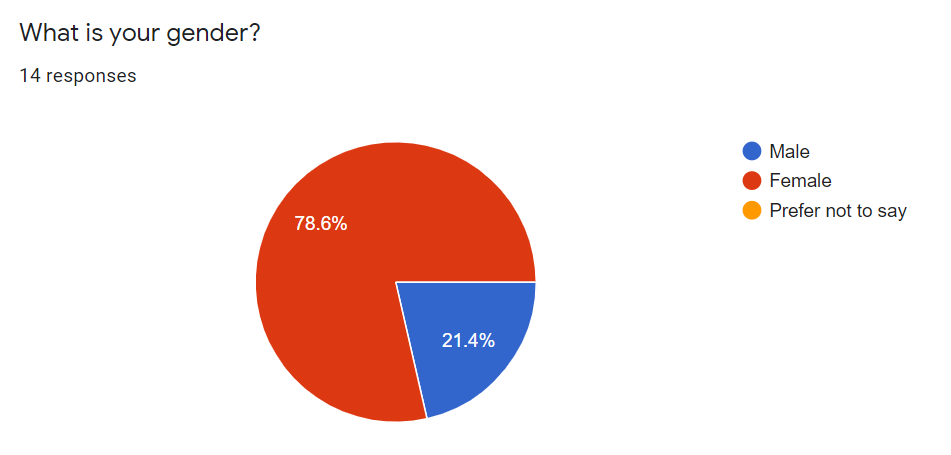
The respondents skewed female, which was also true when I conducted the Working With a Sitting Disability Survey.
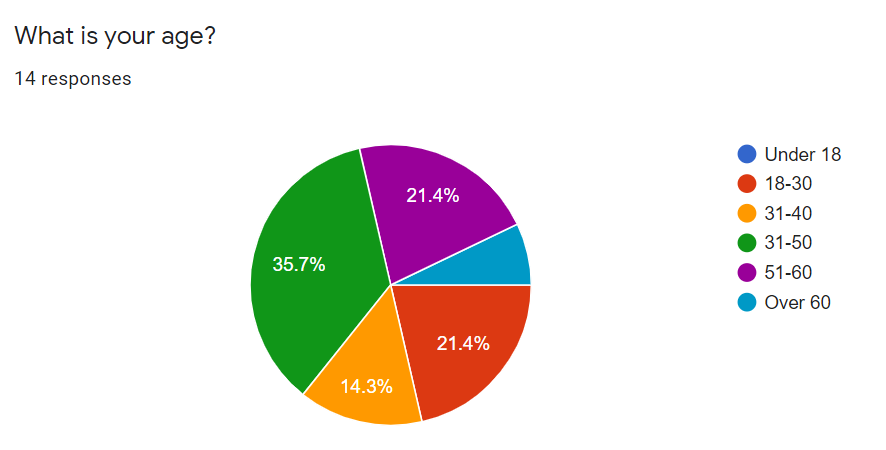
Participants were fairly well distributed in terms of age, although I may have thrown off the survey results unintentionally. I noticed, too late, that I included a typo in the question. The age brackets included both “31-40” and “31-50.” Not surprisingly, 31-50 was the most common age bracket.
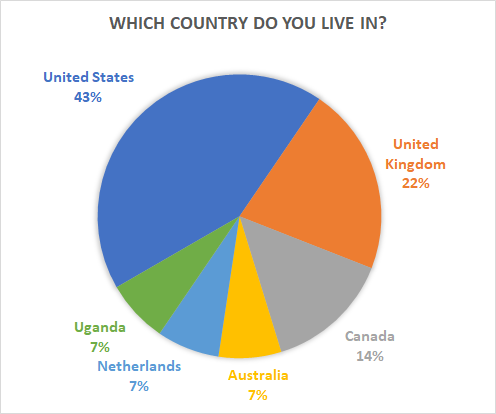
The geography of the respondents was skewed toward English-speaking countries, which is understandable, considering the survey was in English.
Final Thoughts
Many participants expressed their frustration both with their sitting disability, and with others’ reaction to it. “It’s destroyed my life,” wrote one respondent. “It’s damned depressing,” said another.
Some were frustrated by the lack of attention sitting disabilities have received, and how this affected their ability to work within existing systems.
- “This is a totally overlooked disability and no one ever really gets it.”
- “I really wish I had been considered disabled and approved for disability income but I was recently told I was in fact not disabled and my application rejected.”
- “I wish the medical profession knew about this condition as I knew nothing and I felt bad that I couldn’t do something as simple as sitting. I actually felt a failure when I didn’t improve with physio, etc.”
I empathized with these sentiments. I remember feeling like a uniquely tricky case after the Mayo Clinic discharged me without a diagnosis, and my second physical therapy clinic fired me as a patient. How can a person flunk out of medical care?
Then I read up on back treatment statistics and sitting disabilities and realized I wasn’t unique. Rather, the medical system was uniquely unsuited to dealing with patients like me.
I still regularly go through phases of bitterness, despondence, and grief, over the life that might have been. At these times, it would be an understatement to call my situation “damned depressing.”
One individual looked past the doom-and-gloom, and offered a great suggestion which I, unfortunately, do not have the power to enact. They noted, “Amtrak Sleeper units are cost prohibitive, but would change my life if affordable.”
It would be a magical world indeed if I could recline comfortably in a train car during travel, rather than jamming myself into a tiny airplane seat or enduring a cross-country car ride. Alas, Amtrak does not have a history of making my dreams come true.
The results of this survey give me a better framework within which my own actions, preferences, and capabilities can be viewed. I hope others with sitting disabilities will find some comfort in this as well.
Very well done. Extend and publish your findings!!!
Interesting survey. I don’t think most people with sitting probles realize how complex our problems can be.
I lived with a sitting condition for 9 years, too many treatments to mention and a botched surgery before finding my solution.
I had piriformis syndome, and it wasn’t until I found Dr. Tim Tollestrup who pioneered the piriformis muscle removal surgery, and I had my PFCN neurectomy surgery that I was able to sit again. No more anxiety about sitting and no more deep horrific pain when sitting.
I highly suggest a MRN (MR neurography) done at a university hospital and then images sent to Dr. Chhabra at University of Texas Southwestern to be read by him because his eyes can see more than most radiologists. I suggest this because what I have seen is people tend to have more than one problem causing their sitting problem, especially when they have suffered a very long time. Piriformis Syndrome is the most under-diagnosed misunderstood sitting condition ever. And the cure exists for PS now. There’s currently three surgeons doing this surgery. They can also do surgery for pudendal nerves that cause sitting pain.
Also people may have been misdiagnosed. just because something shows up on your MRI doesn’t mean it is the root cause of your pain.
With what everyone has gone through with their sitting problems, what is one more scan? Wouldn’t it be worth it to check out?